“Dreamtime lover comes to me, helping me to clearly see all I truly need to know— your love for me you always show.
Guiding me to do what’s right, giving me strength and insight. Physically separate but living as One, teaching me what needs to be done.
Knowing our love only grows and can never end, as you assist me gradually to my Self mend.”
Have you ever woken with your body humming, breath quickened, heart strangely full? A dream so vivid, it left you aching—or glowing—with something you couldn’t quite name?
So many whisper it quietly: “I had the most intense dream last night… but I can’t tell you. It’s too much.”
But I say, tell me everything. Because these dreams? They are sacred. They’re not just about sex. They are about energy. Integration. Memory. Reclamation.
We give this energy so many names: sexual energy, creative energy, Kundalini, God, Goddess, Great Spirit, Divine Union, Reiki, Seichim, Universal Life Force. But they are all rivers feeding the same source – the wild current of life itself. And its most ecstatic, alchemical expression? Orgasm. There’s a reason we cry out “Oh God” in those moments of deep pleasure. It’s not blasphemy. It’s a soul-deep remembering.
In dreams, anything becomes possible. We may find ourselves in the arms of a stranger, a past lover, someone we’ve never touched in waking life, but who feels as familiar as our own breath. Sometimes we merge with spirit beings, ancestors, archetypes. The forms may be surreal, symbolic, or shapeshifting, because dream lovers aren’t always literal, they’re invitations.
Invitations to reunite with soul threads. To embody the Lover, the Serpent, the Priestess, the Healer. To meet ourselves in forms we’ve long silenced or disowned. Often, it’s not about the person at all, but what they represent. Power. Passion. Tenderness. Permission. The dream body remembers what the waking mind forgets.
And let’s name the deeper truth now: soul-level communion is real. These dreams don’t always stay contained in the psyche. Sometimes, they’re shared experiences. If you’re thinking of someone with strong emotion, longing, desire, even grief, that thought becomes energy. It moves. It reaches. And if the other is attuned to you, they may feel it. Not as a conscious thought, but as a subtle frequency. A stirring in the night. A dream they can’t quite shake.
This is the intelligence of the soul field. Where time and space dissolve. Where lovers remember each other through the veil.
These dreams often arrive during times of emotional or energetic opening. When we’re grieving, creatively blocked, repressing desire, or navigating a threshold, these dreams come as messengers. They bring healing. They activate dormant parts of the body. They offer closure, clarity, confirmation. They reignite our connection to joy, to power, to the sacred yes of aliveness.
Even dream-orgasms, yes, they’re real, can be profoundly healing. Especially if touch, pleasure, or intimacy has been absent in waking life. And yet so many carry shame. They wake from these dreams wondering, “What’s wrong with me?” Especially if the imagery was strange, forbidden, or “inappropriate.” But erotic dreams don’t come to shame us, they come to liberate us.
We’ve all dreamt of partners we wouldn’t choose in the light of day, same-sex lovers, celebrities, even people from our past we’d rather forget. But dreams are symbolic. They’re the soul’s poetry. They speak in images, sensations, and metaphor. And they ask us not to judge, but to listen.
What part of me does this represent? What wants to be felt, healed, or reintegrated? What am I being invited to remember?
Erotic dreams are not just about sex. They’re about wholeness. They’re about power reclaimed. They’re about love, sometimes for another, often for the self. And sometimes, they are simply about joy. And that, too, is sacred. So next time your dream lover comes bearing fire, welcome them. Feel what wants to be felt. Honour what wants to be healed. And if you wake with tears, a sigh, or a sweet ache that lingers into the day, know this:
It wasn’t just a dream. It was a remembering.
📚 Further Reading & Exploration
Robert Moss – Conscious Dreaming On dream travel, soul connection, and shared dreaming experiences.
Barbara Brennan – Hands of Light A classic text on energy fields, cords, and how emotion/thought affects others.
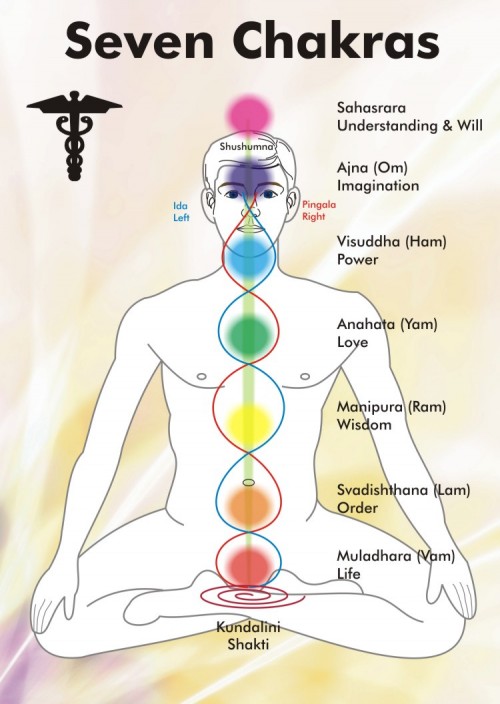
Anodea Judith – Wheels of Life A deep dive into chakras, creative/sexual energy, and inner integration.
Toko-pa Turner – Belonging: Remembering Ourselves Home On the sacred art of dreamwork and returning to the soul’s truth.
Clarissa Pinkola Estés – Women Who Run With the Wolves Archetypal stories that explore feminine psyche, longing, and reclamation.
Mantak Chia – The Multi-Orgasmic Man/Woman Taoist teachings on sexual energy as sacred and transformative force.
Rupert Sheldrake – Morphic Resonance A scientific view of non-local connection and shared fields of experience.
🌕 Ever had a dream that left your soul stirred and your body buzzing? I’d love to hear. Drop a note in the comments or share this with someone who dreams in symbols too.
For many of us, simply being present, fully here, right now, is one of the greatest challenges we face. In Western culture especially, we’re conditioned to think in linear terms: past, present, future. We track what has been, plan what’s next, and often measure our lives by where we’re going and what we hope to achieve. We make lists, set goals, and feel comforted by having a plan. But underneath it all, we may be reacting not to what’s real, but to a story we’ve told ourselves about how things should go.
My mum, bless her, was the Queen of Organisation. With four children and a job, she had to be. Each of us had assigned chores, and our weeks were structured down to the minute. I grew up knowing exactly what I’d be doing, and when. While life still threw curveballs, I found the predictability comforting. When I became a mother myself, I quickly saw how being organised helped ease stress, and that habit carried over into my work life.
Over three decades in the legal industry only reinforced that rhythm. Planning ahead, meeting deadlines, staying in routine, all of it created a sense of order in what was often a stressful environment. But over time, the rhythm became a rut. I began to feel stuck, drained of joy, and quietly suffocated by the very structure that once kept me afloat. I also realised that when organisation becomes too rigid, it stops being helpful. It becomes control.
As I deepened in awareness, I started to sense that time, at least as we know it, might not actually exist. That all time is now. That things unfold not when we want them to, but when the energy aligns. And from that perspective, life became gentler. I stopped expecting things to go a certain way, and with that, emotional reactions softened. I found myself detaching, from outcomes, from expectations, from old habits of control.
I made fewer plans. “Going with the flow” evolved into being the flow. I became more spontaneous. I let things go if they weren’t working, and trusted that something better might be waiting to fall into place. The most I now plan is a basic outline, one day at a time. As for those job interview questions like, “Where do you see yourself in five years?”, I’ve come to see them as part of a cultural story that often robs us of presence, creativity, and possibility. How can we know what five years will bring? Sometimes, we don’t even know what the next five minutes will bring.
I learned the hard way: plans rarely go according to plan.
Now, if something I want to do just isn’t flowing, I don’t push it. If the energy is not aligned, I let it be. I’ve noticed how stressed people get when things don’t go “according to plan”, the frustration, the disappointment, the tension it can cause in relationships. But often, those delays or disruptions are gifts. Protection. Rearrangements. Or just not the right time yet. The puzzle pieces aren’t in place. And when they are, everything clicks.
I thought I had this all sorted. Skeletal plan? Check. Present moment awareness? Check. Calendar reminders so I didn’t forget the essentials? Check. It was working beautifully, until one day when I found myself in a situation where communication had been unclear, and I didn’t know what I was “meant” to be doing next. I’d been told one thing, then it suddenly changed. I felt confused, unprepared, and frustrated.
Old habits kicked in: irritation, storytelling, the mental narrative of how it should have been communicated differently. And underneath it all, discomfort. My little comfort zone, small as it was, had been nudged.
Then came the gentle wisdom of another: Does it really matter what you are doing next?
In that moment, I had to laugh. Who was creating the confusion? The person who hadn’t communicated clearly? Or me, reacting to a story in my head, projecting into the future, and leaving the present moment behind?
It was such a simple lesson, offered in such an effective way: Just show up. Be present. Do what’s needed in the moment of now. Let go of the rest.
“Dreamtime visions speak to me of the truth within,
Wisdom, Healing & Knowledge of Self to me they bring,
Helping me to know the true essence of my Soul,
enabling me to consciously experience
I AM …. One with the Whole.”
There is a life force running through all things. Some call it God, Spirit, Nature, Love, or Universal Energy. The name is less important than the feeling it brings and the healing it makes possible. When we remember this force, we begin to remember who we truly are.
For me, this energy first introduced itself through Reiki and later deepened with Seichim—two distinct yet connected frequencies of the same sacred current. Reiki is often associated with the Japanese lineage, while Seichim flows from Ancient Egypt, through the teachings of Sekhem and the energy of the fierce and compassionate goddesses Sekhmet and Kwan Yin.
Where Reiki is the wave flowing in, Seichim is the wave flowing out. Together, they form a complete cycle of energetic restoration.
A Multi-Layered Being
This healing work finds deep resonance with the Anthroposophical perspective of Rudolf Steiner, which sees the human being as a fourfold being:
Physical Body: The visible body, a map of our accumulated experiences and emotions.
Etheric Body (Energy Body): The life or breath body, responsible for vitality, healing, and rhythm. It thrives on sleep, air, water, nutrition, and nature.
Astral Body: The seat of memory and emotion. When the etheric is weakened, the astral can push through into the physical and cause dis-ease.
Core Self or “I AM”: The indwelling essence of who we truly are – divine, wise, and whole. This is not a “higher” self-perched on some pedestal, but the deepest truth of our being, right here, embodied. The notion of a “higher” self can often reinforce hierarchical thinking rooted in outdated paradigms. In truth, we are not reaching upward, we are remembering inward.
Further expanded by Barbara Brennan, this system includes seven energetic layers beyond the physical—each interpenetrating the other:
Physical Body
Etheric Body
Emotional Body
Mental Body
Astral Body
Etheric Template
Celestial Body
Ketheric Template
Each is linked to a chakra and vibrates at a unique frequency. Some healers also experience more than the standard seven chakras.
Blockages, Breath and the Map of the Body
In Reiki, Seichim, and Body-Based Counselling alike, imbalance and illness are seen to originate from energetic blockages—areas where life force energy cannot flow due to past trauma, grief, fear, suppressed emotions, or limiting beliefs. These imprints are stored in the subtle layers surrounding and entering the body.
When breath and awareness are consciously brought into these wounded areas, subconscious memories surface, and with them, release. In this process comes healing, insight, and a return to flow.
Brennan observed, “Illness is a result of imbalance, and imbalance is a result of forgetting who you are.” Others such as Baginski and Sharamon see symptoms as messages needing to be heard, accepted, and integrated before true healing can occur.
While approaches like CBT (Cognitive Behavioural Therapy) may assist some individuals in reframing thoughts and behaviours, they often stay in the mental realm. Deep transformation, however, often requires feeling, not just thinking. Jamie Sams says to feel is to heal. When emotion is acknowledged and expressed, the energy that has been held or suppressed is free to move again.
The Healing Power of Breath
When our bodies become stressed from pressure or anxiety, the adrenal glands release adrenaline. This hormone increases our heart rate to prepare for a fight-or-flight response. While this is a natural survival mechanism, it has side effects—particularly on the breath.
When we are anxious, our breathing becomes shallow. This reduces oxygen intake and can lead to fatigue, panic attacks, emotional distress, headaches, muscle tension, and even exacerbate conditions like PTSD.
Breath is life. It delivers oxygen to our cells and removes carbon dioxide, a key toxin. You can live without food or water for a time—but without oxygen, only minutes. Breath is also how we move life force energy. When pain is present, intentional breath can ease it. As infants and children, we naturally breathed into our bellies. But over time, many of us begin to breathe only into the upper chest, especially under stress.
Chest breathing results in irregular, rapid breaths. This reduces oxygen flow and limits the body’s ability to exhale toxins. The result? Fatigue, anxiety, and disconnection. The good news is: this pattern can be unlearned.
The Benefits of Cyclic Deep Breathing
Stimulates the lymphatic system, aiding detox and healing.
Strengthens immunity by supporting the body’s self-healing capacity.
Balances brain hemispheres and calms the nervous system.
Reduces anxiety and helps regulate emotional response.
Can be practiced anywhere, at any time, with no tools required.
A Gentle Word on Limitations
If you have asthma or another respiratory condition, cyclic breathing may not be appropriate. Please seek medical advice before practicing.
What Is Cyclic Breathing?
Cyclic breathing is a technique to calm the body and mind during times of stress, anxiety, or fear. One simple and accessible method is based on the Ho‘oponopono rhythm:
Sit comfortably, feet on the ground. Place your hands on your lap or your belly.
Notice your breath, just as it is.
Then begin to breathe in for a count of seven.
Hold for a count of seven.
Exhale for a count of seven.
Hold again for seven.
This is one round. Repeat it seven times.
You may also modify the count to suit your capacity. For example:
Inhale for 3, hold for 3, exhale for 3, hold for 3.
Or: Inhale for 3, hold for 3, exhale for 5, hold for 5.
Breathe slowly and gently, always staying within your comfort zone.
With consistent practice, abdominal breathing becomes natural again. You’ll notice your belly rising and falling as you breathe—just as it did when you were a child.
To support this, try practicing three times a day, or as needed. Repetition is key. Studies suggest it takes around 21 to 30 days to form a new habit. But the benefit is lasting: your body begins to remember the way home.
Enter, Exit, Behold: The Body Speaks
Body-Based Counselling draws on these same principles, using methods that access subconscious information directly through the body. Artistic therapies such as:
Clay work
Watercolour painting
Movement and gesture
Colour exploration
These tools bypass the analytical mind. Through simple yet profound methods like Enter, Exit, Behold, clients can step into a bodily sensation or pain, observe what wisdom it carries, and exit with the insight and resource needed for integration, without being overwhelmed or re-traumatised by the original emotion.
This process allows even unspoken or inexpressible emotions to be seen, shaped, and shifted. Pain takes form in clay. Breath is freed through movement. Colour returns to drawings that once looked lifeless. The intangible becomes tangible. Healing begins.
Real Lives, Real Healing
Here are a few examples that reflect the potency of these approaches:
A woman preparing for breast surgery received six sessions while also working with a naturopath. Just before the operation, scans revealed that the lumps had vanished.
A pregnant woman, leaking fluid after a medical procedure, came to me in a vision asking for help. I sent healing and saw the hole in the sac close. Two weeks later, she had stabilised.
A newborn boy with lung issues was hospitalised. After a brief hands-on healing session, he was released the next day. He later grew into a healthy twelve-year-old.
I lived with knee pain for seventeen years after a traumatic accident. Following my Reiki and Seichim attunement, I released grief I didn’t even know I was carrying. The pain disappeared.
The Counsellor’s Role
Just like with energy healing, true transformation in counselling comes when the client is ready and willing. The counsellor or practitioner simply creates a safe and sacred space, offers guidance, and teaches tools. But the work, the choice, the healing, comes from within.
Permission is essential. Unless a person asks, the energy cannot flow to them. Healing respects free will. When someone is ready and willing to receive, the field opens. Our role is to hold the space — not to push or fix, but to witness and support.
We do not fix. We empower. We do not impose. We invite.
Signs of Change
Change reveals itself in many ways: a client enters hunched, disconnected, anxious. After the session, they stand taller, breathe deeper, feel lighter. Art becomes more vibrant. Clay forms soften. Colour returns to the canvas. Their posture changes. So does their presence.
That is healing. That is remembering.
“The energy knows the way. All it needs is your yes.”
Social struggles throughout history have been instrumental in implementing human rights legislation, changing existing laws, and shaping societal thinking about personal freedoms. One of the longest and most contested of these struggles is the fight for women’s reproductive and contraceptive rights. The debate surrounding women’s autonomy over their bodies and their right to access abortion services has persisted for centuries, driven by ethnocentric, patriarchal, and religious moral perceptions, as well as by gendered stereotypes and legislative control.
The issue of abortion rights has repeatedly highlighted the tension between personal autonomy and state, religious, and medical authority. Despite advancements in women’s rights movements and international human rights frameworks, such as the Universal Declaration of Human Rights (United Nations n.d.a) and the Convention on the Elimination of All Forms of Discrimination against Women (CEDAW) (UN Women 2000-2009), barriers to reproductive freedom remain entrenched in many societies. The historical and ongoing struggle for reproductive rights, particularly the right to safe and legal abortion, reveals the enduring power dynamics that seek to control women’s bodies and choices, and demonstrates that achieving genuine gender equality remains an unfinished global challenge.
The Overturning of Roe v. Wade: A Landmark Moment
Women’s autonomy over their bodies has caused an ongoing heated societal debate for centuries. The latest major event occurred in 2022 with the overruling of the 1973 Roe v. Wade decision by the United States Supreme Court on 24 June 2022 (Clough 2022; Lewandowska 2022). The outcome of Roe v. Wade was that the “Fourteenth Amendment’s concept of personal liberty and restrictions upon state action . . . is broad enough to encompass a woman’s decision whether or not to terminate a pregnancy” (Roe v. Wade 1973, at 153). Abortion could now occur in other circumstances (Ehrlich 2018; Ginsberg 1985). Previous law stated termination could only occur if a woman were pregnant due to rape or incest, where there were fetal anomalies, or where the mother’s life was at risk (Ehrlich 2018; Ginsberg 1985).
The overruling of the Roe v. Wade precedent in 2022 has global implications concerning women’s health. It is an attack on human reproductive rights as it removes “the constitutional right to bodily autonomy from over half the United States population” (Clough 2022, p.160; Lewandowska 2022; Cherminsky 2022; The Lancet 2022). As Clough (2022, p.160) states, “it serves as a stark reminder of the need to defend human rights; it is not enough to assume that, once granted, they cannot be taken away.”
Historical Context: Slavery and Early Abortion Legislation
To understand the abortion debate, changes to legislation, and the struggle for women to access abortion services, we need to revisit the 1800s when white people owned Black slaves and relied upon slaves for cheap labour and economic growth (Murray 2021). The prohibition of the importation of slaves into America in January of 1808 (Murray 2021) resulted in slave owners concerning themselves with the “reproductive capacities of enslaved women” because the source of their labour and economy now needed to be procured from slaves’ children (Murray 2021, p.2034). Enslaved women were aware that any child they bore was not rightfully theirs and could be sold (Murray 2021). Therefore, women used various techniques to inhibit conception or abort their unborn child (Murray 2021).
As a consequence, “slave owners sought to deter and punish efforts to prevent or terminate pregnancies” (Murray 2021, p. 2035). Abortion began to be criminalised, and legislation was passed that banned the distribution of contraceptives and abortifacients, which had not been banned prior to the aforementioned 1808 legislation (Murray 2021; Siegal 1992).
Medical Campaigns and the Criminalisation of Abortion
The campaign to enact anti-abortion legislation was primarily organised by white male physicians who considered contraceptive information provided to all women and actions by female Black and Indigenous women as dangerous (Goodwin 2020; Joffe, Weitz & Stacey 2004). Further, these physicians perceived abortions, if allowed to continue, as a disruption of the American social order of motherhood, family, and white dominance due to birth rates amongst white women decreasing (Beisel & Kay 2004; Murray 2021; Ehrlich 2018).
In 1857, Dr. Horatio Storer, a “Harvard-educated gynaecologist,” spoke at a “meeting of the Suffolk District Medical Society” (Ehrlich 2018, p. 182). He addressed the issue of an “alarming frequency of induced abortions among respectable Protestant women…” (Ehrlich 2018, p. 182). Storer convinced “the Boston medical society and the then recently founded American Medical Association (AMA) to establish investigative committees to look into ‘criminal abortion’ to suppress what he perceived to be ‘the slaughter of countless children now perpetuated in our midst’” (Ehrlich 2018, p. 182). Storer believed women’s physiological makeup rendered “her incapable of self-management” (Ehrlich 2018, p.185).
The AMA’s campaign to criminalise abortion was based on “a paternalistic and racialized code of white-male moral authority over women’s reproductive bodies” (Ehrlich 2018, p.183). The campaign resulted in abortion becoming a statutory crime in all states of America by the end of the nineteenth century unless certification by a doctor occurred that the procedure would “save the life of the pregnant woman” (Ehrlich 2019, p.183). Abortion laws now existed that mirrored eugenic concerns regarding controlling reproductive rights due to fear-based perceptions that white women were not producing offspring as rapidly as immigrants and non-whites (Murray 2021; Ehrlich 2018).
Contemporary Efforts to Restrict Abortion Rights
The racially motivated and gendered paternalistic and religious views regarding abortion reveal the true impetus for criminalisation and explain, to some degree, why efforts still remain globally by men to legally control women’s bodies and choices as per the following examples:
2017 America: “Unprecedented attacks on reproductive health rights” resulted in 19 states adopting “63 new restrictions on abortion rights, service provision, and patient access” (Espey, Dennis & Landy 2018, p. 67).
2018 Argentina: A bill to decriminalize and legalize abortion was debated in Congress for the first time but did not pass through the Senate (Sutton 2020, p.1).
Access to abortion in America since 1976 has undergone further restrictions with increased waiting periods, biased counselling, and a mandate regarding parental involvement for minors (Joffe, Weitz & Stacey 2004; Grossman et al. 2014a; Grossman et al. 2014b; Minkoff, Diaz-Tello & Paulk 2021; Askola 2018).
Texas, May 2013 to November 2013: A decrease by half in the facilities where medical abortion was available (Grossman et al. 2014a; Grossman et al. 2014b).
Australia: While surgical abortion has been provided as a health service “since the early 1970s,” medical abortion utilising Mifepristone “was deliberately obstructed” by the Federal Government via legislation concerning its authority over pharmaceutical drug importation, and it was not until 2006 that the legislative restriction was removed (Baird 2015, p.169). It took until 2012 for Mifepristone to be approved by the Australian Federal Government as a commercial import, and it was not until 2013 that it became a listed subsidised medicine (Baird 2015).
Reproductive Healthcare and Rights in Queensland: A Complex Landscape
Reproductive healthcare in Queensland is shaped by a complex interplay of legal, ethical, and social factors. The state has seen significant changes, particularly in the areas of abortion rights, fertility treatments, and workplace reproductive rights. These issues reflect broader societal debates around personal autonomy, healthcare access, and the role of government in regulating reproductive choices. However, despite legislative progress, significant barriers remain, especially for those in rural and remote areas.
Decriminalisation of Abortion
In Queensland in 2018 a pivotal step occurred in recognising reproductive autonomy, aligning the state with the broader Australian movement to treat abortion as a healthcare issue rather than a criminal matter (Storry, 2018). While the legal framework shifted, practical access to abortion services remains uneven. Women in rural and remote areas face considerable obstacles, such as long distances to clinics, financial barriers, and a lack of available healthcare professionals (Sexual Health, 2022).
The Termination of Pregnancy in Queensland Post-Decriminalisation Study (2022) indicates that while decriminalisation aimed to improve access, stigma surrounding abortion remains a significant challenge. In smaller, more conservative communities, social pressures often prevent women from seeking services. According to Deveny (2023), these social and cultural factors, combined with logistical challenges, continue to hinder women’s access to reproductive health services.
Workplace Reproductive Rights
Workplace protections for pregnant employees have been a subject of continued evolution in Queensland. The state’s legislative changes concerning maternity leave, workplace discrimination, and the prevention of gender-based discrimination provide a more supportive framework for women. However, Deveny (2023) highlights that discrimination in the workplace remains a persistent issue, and women often face barriers to achieving full reproductive rights in the workplace, particularly in industries that are male-dominated or conservative.
The Queensland Government, under Premier David Crisafulli, has recently implemented a significant policy regarding abortion legislation. In December 2024, Premier Crisafulli introduced a parliamentary motion that effectively bans any changes to the state’s abortion laws until at least October 2028. This action was taken to uphold his election promise of no alterations to abortion laws and to prevent potential legislative challenges from within his own party. The motion passed despite opposition from the Labor Party, which voted against it, expressing frustration over the move (The Australian, 2024).
This policy has been met with criticism from various quarters. Opponents argue that it undermines the democratic process by restricting Members of Parliament from debating and introducing bills on the subject, thereby limiting legislative scrutiny and public discourse on reproductive rights (Courier-Mail, 2024).
Additionally, for a critical analysis of Premier Crisafulli’s decision to restrict parliamentary debate on abortion, you may find the article “The deeper issue behind Premier’s move to gag abortion” from The Courier-Mail insightful (Courier-Mail, 2024).
The decriminalisation of abortion in Queensland in 2018 marked a significant step in recognizing reproductive autonomy (Storry, 2018). However, practical access to abortion services remains uneven, with women in rural and remote areas facing considerable obstacles such as long distances, financial barriers, and a lack of healthcare professionals (Sexual Health, 2022).
Recent discussions in Queensland have also focused on the need for reproductive health leave to support women undergoing fertility treatments or coping with miscarriage (McKell Institute, 2024). The introduction of such leave would improve employee retention and reduce workplace discrimination, though it has not yet been widely implemented in Australia.
Regulation of IVF and Assisted Reproductive Technologies (ART)
In a related issue, the regulation of ART remains contentious in Queensland, particularly concerning ethical issues related to donor anonymity and the rights of donor-conceived children. The lack of a national donor registry has led to inconsistent standards and raised ethical questions about how embryos and donor information are handled (Messenger, 2024).
Global Influences and Local Impacts
Global trends in reproductive rights, such as the overturning of Roe v. Wade in the United States, have sparked concerns in Queensland about the potential erosion of local reproductive rights, especially in rural areas with entrenched conservative values (Murray, 2021). This highlights the need for continued vigilance in defending reproductive rights, both locally and globally (Clough, 2022).
International Implications: A Global Struggle
While the fight for reproductive rights is deeply embedded in Australia’s political landscape, the battle rages on beyond our borders, particularly in the United States. Under the current administration of Donald Trump, the reproductive rights of women have once again become a political battleground, mirroring the long history of male-driven control over women’s bodies.
In his first 100 days of a second term, Trump has enacted a series of controversial measures that significantly restrict access to reproductive healthcare. Among these, pardoning anti-abortion activists and reinstating the Mexico City Policy—which restricts foreign aid to organizations that provide or promote abortion—are just the beginning. These actions have ignited fierce opposition from reproductive rights groups who argue that such moves are an affront to women’s autonomy (Harrington, 2023; International Planned Parenthood Federation, 2023).
The administration’s decision to revoke policies supporting military travel for reproductive services and freeze critical funding for low-income patients, particularly affecting Title X clinics, reflects a deliberate rollback of essential healthcare provisions (Guttmacher Institute, 2023). Adding to the growing alarm, the Trump administration has been accused of failing to support families through comprehensive, family-friendly policies, while paradoxically championing pro-natalist stances (Smith, 2023).
Perhaps most concerning, however, is the increasing possibility of restrictions on abortion medications, such as mifepristone, which could have far-reaching consequences for women seeking access to safe and legal abortion care (American Medical Association, 2023). For many in the United States, these policies are a painful reminder of the historical attempts to control women’s reproductive choices. The echo of past struggles—of rights denied, and freedoms curbed—is unmistakable.
The response from American reproductive rights groups is growing louder, as they seek to not only protect access to healthcare but to remind the world of the consequences of turning back the clock on women’s bodily autonomy (Planned Parenthood, 2023). These developments serve as a stark reminder that the struggle for reproductive rights is ongoing, not just in the halls of power in Australia, but across the globe.
International Human Rights and the Struggle for Reproductive Rights
Beyond Debate: Reproductive Rights Are Human Rights
It is frankly incomprehensible that in the 21st century, women still have to fight for their reproductive rights. The fact that the United Nations had to establish a convention affirming these rights — as if women’s autonomy over their own bodies needed external validation — underscores how deeply ingrained patriarchal control remains. Under Article 12 of the Convention on the Elimination of All Forms of Discrimination Against Women (CEDAW 1979), all State Parties, including the United States, Australia, and Argentina, are obligated to ensure women have access to health services, including those related to family planning, on the basis of equality.
In conclusion, the very existence of a United Nations Convention on the Elimination of All Forms of Discrimination Against Women (CEDAW) raises a confronting question: why was such a Convention even necessary? Are women not human? Shouldn’t their rights be inherently protected as human rights? The answer lies in centuries of systemic inequality and the ongoing disregard for women’s autonomy, dignity, and agency.
Even today, despite many nations ratifying CEDAW, its principles are too often ignored or selectively applied. Unfortunately, many political leaders and pro-life groups continue to undermine women’s rights, placing personal beliefs and ideological agendas above the basic rights to health, autonomy, and equality. These groups and individuals are not the ones who will endure pregnancy, give birth, or raise a child. While some men may contribute to these responsibilities, the physical, emotional, and social realities of these experiences overwhelmingly fall to women. Those who seek to control women’s reproductive choices — including decisions around accessing termination services — have no place dictating healthcare policy or harassing women at clinics. It is particularly reprehensible when those women being harassed may not even be attending for a termination.
These ongoing struggles — where women’s voices are disregarded, silenced, or treated as secondary — make it painfully clear that, despite what should be a simple truth, women’s rights are still viewed by many as negotiable. The very fact that we need a global framework like CEDAW to attempt to safeguard these rights is a stark reminder of how far we have yet to go. Until all women are treated as equal, autonomous human beings — with full control over their bodies, lives, and choices — the fight for equality and dignity remains not just necessary, but urgent.
However, the lived reality is one where women’s reproductive autonomy is continuously undermined and politicised by politicians in positions of patriarchal governance, alongside pro-life advocates who, while not making the political decisions, relentlessly harass women who choose to terminate a pregnancy. These politicians, who will never bear the physical, emotional, social, or financial consequences of pregnancy and childbirth, continue to make decisions on behalf of women — often based on the influence of votes from pro-life groups whose members stalk and harass women seeking services, regardless of whether they are attending a clinic for a termination or another medical reason. This persistent disregard for women’s right to choose and control their own reproductive health must be recognised for what it is: a denial of basic human rights.
American Medical Association, 2023. Mifepristone Restrictions: The Impact on Women’s Health. [online] Available at: https://www.ama-assn.org/2023-mifepristone [Accessed 1 May 2025].
Baird, M. (2015) ‘Obstacles to abortion access in Australia: The case of Mifepristone’, Australian Health Review, 39(2), pp. 168-172.
Beisel, N., and Kay, A. (2004) ‘The social construction of abortion: Race, class, and the politics of women’s rights’, Gender and Society, 18(2), pp. 123-139.
Cherminsky, V. (2022) ‘The United States Supreme Court’s overturn of Roe v. Wade: A profound setback for women’s reproductive rights’, The Journal of Constitutional Law, 34(1), pp. 45-63.
Clough, M. (2022) ‘The end of Roe v. Wade: A world of reproductive injustice’, The Journal of Women’s Health, 31(1), pp. 156-162.
Ehrlich, J.S., (2018) ‘Abortion in America: The history of reproductive rights and their legislative battles’, Journal of Gender Studies, 29(2), pp. 180-195.
Espey, E., Dennis, A., and Landy, R. (2018) ‘Unprecedented attacks on reproductive health rights in the United States’, American Journal of Public Health, 108(1), pp. 67-72.
Goodwin, S. (2020) ‘The criminalization of reproductive autonomy: History and impact of anti-abortion legislation’, International Journal of Reproductive Rights, 5(1), pp. 112-118.
Ginsberg, A. (1985) ‘The impact of Roe v. Wade on the reproductive rights movement’, Reproductive Health Journal, 22(3), pp. 25-33.
Grossman, D., et al. (2014a) ‘The impact of restricted abortion access in Texas’, American Journal of Public Health, 104(3), pp. 466-472.
Grossman, D., et al. (2014b) ‘Effect of reduced abortion access in Texas: The influence of restrictions on reproductive healthcare’, Reproductive Health Matters, 22(44), pp. 78-85.
International Planned Parenthood Federation, 2023. Mexico City Policy: The Global Effects of Trump’s Abortion Restrictions. Available at: https://www.ippf.org/mexico-city-policy [Accessed 1 May 2025].
Joffe, C., Weitz, T., and Stacey, C. (2004) ‘Abortion access: The limits of legal reform’, Social Science & Medicine, 58(10), pp. 1991-2000.
Lewandowska, M. (2022) ‘The rise of reproductive injustice: A critique of Roe v. Wade’s overturn’, Global Feminist Review, 24(1), pp. 139-146.
Minkoff, H., Diaz-Tello, F., and Paulk, S. (2021) ‘Abortion laws: A global comparative analysis of reproductive health policies’, Journal of International Women’s Health, 38(2), pp. 210-220.
Murray, J. (2021) ‘The intersection of race, gender, and reproductive justice in 19th century America’, Women’s Studies Quarterly, 49(4), pp. 2030-2040.
Roe v. Wade (1973) U.S. Supreme Court Case, 410 U.S. 113.
Siegal, R. (1992) ‘The erosion of abortion rights in America: The history and politics of anti-abortion movements’, American Political Science Review, 86(1), pp. 50-65.
Smith, D., 2023. Trump’s Pro-Natalist Agenda: The Contradiction in Family and Reproductive Policies. The New York Times. Available at: https://www.nytimes.com/2023/trump-pro-natalist [Accessed 1 May 2025].
Sutton, L. (2020) ‘Abortion law in Argentina: The fight for reproductive justice continues’, Journal of Latin American Politics, 41(2), pp. 1-8.
The Lancet (2022) ‘The implications of the end of Roe v. Wade for reproductive rights’, The Lancet, 399(10337), pp. 1609-1612.
After seven years away, I’m so pleased to be returning to Dreamwork — a practice that has always held a special place in my heart and soul. While life called me in other directions for a time, the world of dreams, symbolism, and inner landscapes remained a constant, reassuring presence that helped me navigate those years.
During this time, I obtained my Social Work degree, cared for a loved one, and reconnected with my previous career in the legal world. Each of these experiences has continued to shape me, broadened my understanding of human experience, and further deepened my appreciation for the quiet, profound wisdom our dreams offer.
Dreamwork has long been a source of insight, healing, and creative exploration for me and those I’ve worked with. It’s a space where our unconscious speaks in rich images, emotions, and metaphor — and where we can gently unravel meaning, find clarity, and reconnect with parts of ourselves we may have forgotten.
Returning to this practice and sharing dream wisdom feels like coming home. With new skills, fresh perspectives, and a deepened sense of empathy, I am excited to be offering Dreamwork sessions once again, both for those new to exploring their dreams and for those looking to pick up where they may have left off. I am once again available to work with individuals through online consultations via email, phone or Microsoft Teams. Whether you’re looking to explore recurring dreams, uncover deeper meanings, or simply gain clarity from your inner landscape, I would be honoured to assist you in your transformative process.
Thank you for your support, your encouragement, and your presence. I look forward to seeing what this next chapter of Dreamwork holds for all of us.
Older single women in Australia are at high risk of facing a crisis. One brought on by neoliberal ideologies and policies which intersect with gender and wage bias, along with the historical marginalisation of women in a patriarchal society. This crisis is homelessness and why it is exponentially growing can be understood through the lens of feminist standpoint theory and neoliberalism.
Like all theories, feminist standpoint theory has its limitations and uses. It assists with analysing and understanding this particular social justice issue because feminist standpoint theory considers the individual experiences of the women involved. It also takes into consideration women’s historical roles in society. Standpoint theory emerged from Marxism wherein it was seen that members of society who were oppressed were privy to knowledge the privileged class were not aware of (Borland 2020). In 1983 when Nancy Hartsock published her book “Money, Sex and Power” she provided a theoretical method which took into consideration women’s unique perspectives within society (Hekman 1997, p. 341). This theory also justified feminist claims regarding women being oppressed members of society and feminist standpoint theory as a methodology began (Hekman 1997). During the 80s and 90s other contributors to this theory included Sandra Harding, Merrill Hintikka, Patricia Hill Collins and Dorothy Smith (Hekman 1997; Borland 2020). Harding was of the view that even though scientific researchers claimed to be neutral, their research methods and results were sexist (Borland 2020, p.1).
Harding saw that by implementing standpoint theory, it would reveal the power held within ‘scientific authority’ and would create ‘knowledge that is embodied, self-critical and coherent’ (Borland 2020, p.1). Patricia Hill Collins contributed an African American feminist perspective arguing that race, gender, class oppression and lack of privilege for African American women also provided a unique perspective to the feminist landscape which needed to be seen (Borland 2020). Whilst standpoint theory can be seen as essentialist due to the implied belief that a universal female standpoint exists, theorists utilising feminist standpoint theory have chosen to focus on the ‘political aspects of social position’ from a feminist view rather than speaking for all women (Borland 2020, p.1). Use of feminist standpoint theory and practice, however, has come under scrutiny as it appears to challenge the more recent feminist theories which have emerged from ‘postmodernism and poststructuralism’ (Hekman 1997, p.342).
Nonetheless, Hekman (1997, p.342) argues that feminist standpoint theory is based on the understanding that “knowledge is situated and perspectival, and that there are multiple standpoints from which knowledge is produced.” Hawkesworth (1999) sees feminist standpoint theory not as an epistemology but as an analytical tool. Both Hawkesworth (1999) and Hekman (1997) posit there are various types of competing feminist standpoints and that by critically examining those, problems can be illuminated which Hawkesworth (1997, p.152) states …’empirical research must engage’.
When looking at the issue of older single homeless women in Australia some of the specific gender-based factors for this cohort are that their earlier lives have been shaped by the societal norm they would marry and their husband would provide for them in their roles as homemakers, child-bearers and predominantly mothers (Darab & Hartman 2013; Hartman & Darab 2017). According to McFerren & Laverty (2010),a high percentage of older single homeless women have suffered domestic violence or experienced adverse tragedy in their earlier lives. Common themes found in various studies concerning lack of housing security available to these women both now and into the foreseeable future, are cited as being systemic issues; domestic violence; age, wage, employment and gender discrimination; and relationship breakups (McFerren & Laverty 2010;Darab & Hartman 2013; Hartman & Darab 2017; Irwin & Leeson 2016; Sharman 2017; Faulkner & Lestner 2020). Invisibility via research and media representation of this group of women, which results in a lack of service provision specifically tailored for them, along with housing unaffordability, are also cited as being factors which are contributing to the increasing number of older women who are, or are becoming, homeless (McFerren & Laverty 2010; Darab & Hartman 2013; Hartman & Darab 2017; Irwin & Leeson 2016; Sharman 2017; Faulkner & Lestner 2020).
In 2017 Hartman & Darab conducted a qualitative research project using feminist standpoint theory regarding older homeless women and pathways to housing in the rural area of the Northern Rivers, New South Wales. They found intersectionality was occurring between gender, relationship status, aging and lack of home ownership (Hartman & Darab 2017). The absence of employment opportunities combined with minimal public transport were also cited as factors contributing to older single women becoming homeless in the region (Hartman & Darab 2017). Reasons Sharman (2017) gives for the rise in numbers of older single homeless women in her Victorian study are that these women, due to the roles they played earlier in their lives were locked out of the labour market and as such were prevented from accumulating superannuation and savings. Sharman (2017, p.51) also cites ‘adverse critical life experiences’ which are ‘non-normative’, as being a factor. For example, the unexpected death of a partner, ill health, sick children, unemployment or disability all can impact on an individual’s ability to function as they would normally expect to (Sharman 2017).
Other critical life events which Sharman (2017) states have impacted on older single women have been rental increases, mortgagee repossessions, evictions and housing stress brought on by increasing costs where 30 per cent or more of household income is required to secure housing. In addition to the aforementioned factors women’s work is often undervalued, unpaid or underpaid (Sharman 2017; Healy & Kidd 2013). Many women’s working lives are interrupted by children and they are often pushed into the dominant female industries of health, teaching and retail (Sharman 2017). Mostly relying on less pay than male counterparts along with part-time or casual work to meet family responsibilities results in less savings and less superannuation being accumulated by the time they retire (Sharman 2017; Healy & Kidd 2013). Recent research by Faulkner and Lestner (2020) estimated “240,000 women aged 55 or older and another 165,000 women aged 45-54 are at risk of homelessness” in Australia.
Whilst no government is responsible for exceptional individual life experiences, under the United Nations agreements Australia is privy to, the State is responsible for the provision of certain basic human rights to all citizens, which it does not appear to be adhering to. In 1976 Australia ratified the United Nations International Covenant on Economic, Social and Cultural Rights. At Article 11, 1., it states that adequate housing is a fundamental human right (Marston, McDonald & Bryson 2014; Australian Legal Information Institute 1976; Australian Human Rights Commission 1976; Human Rights and Equal Opportunity Commission 1996). The Universal Declaration of Human Rights, which Australia was a founding contributor to in 1948 and signatory of, at Article 25, states, “Everyone has the right to a standard of living adequate for the health and well-being of himself and his family, including … housing” (United Nations 1948).Despite these signed agreements, according to the Australian Bureau of Statistics 2016 Census, there were an estimated “6,866” homeless older women and “5,820” older women who were “living in marginal housing” and “may be at risk of homelessness” (Australian Bureau of Statistics 2017; Australian Human Rights Commission 2019a).
Further, older women are seen to be “the fastest-growing cohort of homeless Australians” evidenced by a 31 per cent increase occurring between 2011 and 2016. (Australian Human Rights Commission 2019a; Australian Human Rights Commission 2019b). Dominant neo-liberal ideology and practices which have been occurring in Westernised countries for the past 30 years are a major factor which impacts on homelessness (Bullen 2015; Hartman & Darab 2017). Neo-liberalism is a mode of governing which emphasises free markets, individuals being solely responsible for themselves and market like modes of service provision (Bullen 2015; Hartman & Darab 2017).
As a consequence of neoliberalism, there has been a shift away from discourses of homelessness being a social issue brought about by unemployment, poverty, domestic violence and disadvantage, to being one of a personal issue (Bullen 2015; Sharman 2017). This has consequently had a detrimental impact on service provision and created negative feelings of self-worth, blame and exclusion for homeless persons (Bullen 2015). Policies implemented, which included the reduction of capital gains tax in 1999 and negative gearing in the late 1980s, have resulted in decreased housing affordability as house prices, compared to available income during the past 15 years, has increased sharply (Hartman & Darab 2017). Further, there has been a decline in public housing availability since the 1990s as the State’s focus has been on offering financial support for low-income earners via rent assistance within the private rental market, as well as implementing the first home owner’s grant, rather than providing public housing (Hartman & Darab 2017).
These policies have resulted in a rental market which favours investors and landlords (Hartman & Darab 2017). Media representation based on neo-liberal principles presents a perspective of homelessness, generally speaking, that some are deserving and undeserving of State assistance (Lyons & Smedley 2020). Those who are considered deserving are those who through no personal fault suddenly find themselves homeless and those who are classed as undeserving are often stereotyped as being slack due to the perception that they are incompetent (Lyons & Smedley 2020). What is missing from media representation regarding homelessness in Australia is a discussion concerning the growing number of single older women who are unable to secure a home (Lyons & Smedley 2020).
Whilst there is not a lot of research available regarding this sector of homelessness specifically, research does validate that a looming crisis is pending. Many factors are contributing to single older women becoming homeless in Australia, not the least of which are neoliberal ideology and practices that are proving to not only be detrimental to a whole generation of women currently but potentially also for women in the future.
Australian Legal Information Institute, Australian Treaty Series 1976, No 5, Department of Foreign Affairs, International Covenant on Economic, Social and Cultural Rights, United Nations, New York, viewed http://www.austlii.edu.au/au/other/dfat/treaties/1976/5.html
Bullen J 2015, ‘Governing Homelessness: The Discursive and Institutional
Construction of Homelessness in Australia’, Housing, Theory and Society, 32:2, 218-239, doi:10.1080/14036096.2015.1024886
Darab, S & Hartman Y 2013, ‘Understanding Single Older Women’s Invisibility in Housing Issues in Australia’, Housing, Theory and Society, vol. 30, no. 4, pp. 1–20, doi:10.1080/14036096.2012.746944
Hartman, Y & Darab, S 2017, ‘The housing pathways of single older non-home owning women in a rural region of Australia’, Journal of Rural Studies, vol. 54, pp. 234–243, doi:10.1016/j.jrurstud.2017.07.003.
Hawkesworth, M 1999, ‘Analyzing backlash: Feminist standpoint theory as analytical tool’, Women’s Studies International Forum, vol. 22, no. 2, pp. 135–155, doi:10.1016/S0277-5395(99)00003-5.
Healy, J & Kidd, M 2013, ‘Gender-based undervaluation and the equal remuneration powers of Fair Work Australia’, Journal of Industrial Relations, vol. 55, no. 5, pp. 760–782, doi: 10.1177/0022185613491683.
Hekman, S 1997, ‘Truth and Method: Feminist Standpoint Theory Revisited’, Signs, vol. 22, no. 2, pp. 341–365, doi:10.1086/495159.
Irwin P & Leeson G 2016, ‘Late Middle-Aged Single Women and The Risk of Homelessness in Rural Australia’, The Gerontologist, vol. 56, no. Suppl3, pp. 719–719, doi:10.1093/geront/gnw162.2932.
Lyons G & Smedley C (2020) ‘The new face of homelessness? Examining media representations of women’s homelessness in five Australian news sources’, Journal of Social Distress and Homelessness, doi:10.1080/10530789.2019.1709269
McFerran, L & Laverty, S 2010, ‘It could be you: female, single, older and homeless’, Parity, vol. 23, no. 7, ISSN:1032-6170
Marston, G, McDonald, C & Bryson, L 2014, The Australian welfare state: who benefits now?, Palgrave Macmillan, South Yarra.
Petersen, M 2015, ‘Addressing older women’s homelessness: service and housing models’ Australian Journal of Social Issues, vol. 50, no. 4, pp. 419–438,458, doi:10.1002/j.1839-4655.2015.tb00358.x.
Sharman A 2017, The Voices of Midlife Women Facing Housing Insecurity in Victoria, Australia, Social Policy & Society, Vol 16, No. 1, pp.49-63, doi:10.1017/S1474746415000603
Australia is a country of polarity and diversity which purports a political ideology of all-inclusive multiculturalism. Yet at the core of the nation lays a foundation of institutional systems built on implicit and explicit conditioning which have their roots in the social construct of ethnocentric racism. The racialisation and othering of those who are not white has emanated from Australian Governments and through media commentary into every aspect of life for Aboriginal and Torres Strait Islander peoples since colonisation. Creating disadvantage, ill-health, intergenerational trauma and a lack of social equity for Indigenous Australians. An example of this racialisation and othering occurred during the public debate surrounding Adam Goodes stance against racism. A situation which could have been better understood and avoided if viewed through the lens of white habitus, cultural responsiveness and anti-racist practice.
Historically, the Social Work profession is not exempt from creating catastrophic racist damage for Indigenous Australians. Issuing an apology to Indigenous Australians in 2004 for the profession’s role in creating inter-generational trauma, it was 2010 before the profession’s Code of Ethics was re-worded to include the ethical principles of social justice, human rights, respect for diversity, and provision of culturally competent, safe and sensitive practice which encompasses a commitment to valuing Indigenous Australians’ knowledge, experience, skills and relationships (International Federation of Social Workers 2018; Australian Association of Social Workers 2010; Green Bennett & Betteridge 2016). The Social Work profession, therefore, have a critical role to play in assisting with the de-colonisation of institutionalised racism.
Since invasion by the British in 1788 ethnocentric implicit and explicit racism, originally based on social Darwinism, has permeated life for Aboriginal and Torres Strait Islander peoples. Racist behaviours have been foundational to the nation’s identity (Sherwood, Osmond & Phillips 2020). Aboriginals were seen by British colonisers to be a dying primitive race who were inferior to the British in culture, biology and morality (Hollinsworth 2006; Sherwood, Osmond & Phillips 2020; Bennett & Green 2019). Racist conditioning occurred by way of social Darwinism being taught to ‘successive generations of non-indigenous (and indeed indigenous) Australians’ resulting in institutionalised racism becoming both explicit and implicit within the Australian psyche (Hollinsworth 2006, pp. 83-84). This type of conditioning and its’ ongoing perpetuation can be understood and also eradicated when viewed from the concepts of Bourdieus’ habitus theory and also Whiteness theory, which when combined create the theory of White habitus (Walter, Taylor & Habibis 2011). Habitus, as seen by Bourdieu involved how people were socially conditioned via habits, dispositions and skills which determine their understanding of a situation and how they respond to it based on the cultural norms they have been exposed to (Emirbayer & Williams 2005; Walter, Taylor & Habibis 2011).
Whiteness theory focusses on and calls for the critical reflection of how white people do not normally see themselves as a race which holds power and dominance over other races (Walter, Taylor & Habibis 2011; Vanidestine & Aparicio 2019). When utilising White habitus, focus is moved away from othering and brought back to self, whilst also revealing how power relations and discourses are racially formed (Walter, Taylor & Habibis 2011; Young 2008). Explicit racism utilised by various Australian governments to maintain white ‘racial homogeneity’, originally involved extensive discursive efforts and repressive legislation to eradicate the country of the existing Aboriginals and their cultures (Sherwood, Osmond & Phillips 2020, p.98; Bennett & Green 2019). For example, in Queensland, legislation was implemented in 1897 via the Aboriginals Protection and Restriction of the Sale of Opium Act which served to codify beliefs that Aboriginals were a dying race, whilst asserting Australia as a white space in which Aboriginals did not belong (Sherwood, Osmond & Phillips 2020). Legislation such as this Act governed every aspect of Aboriginal life; their health, education, employment, housing, the justice system and welfare (Hollinsworth 2006; Briskman 2014; Bennett & Green 2019).
Australia’s institutionalised racism still exists, as was apparent in 2007 when the Howard Government implemented the Northern Territory Intervention, contravening international law in the process (Springer 2007). The Australian Bureau of Statistics (2016) states 2.8 per cent of the Australian population identify as Aboriginal or Torres Strait Islanders and in 2015 to 2016, according to the Australian Human Rights Commission (2017), 54 per cent of the complaints received concerning racism under The Racial Discrimination Act were received by Indigenous Australians. Racist practices, policies and media discourses have had and continue to have a major detrimental impact on Indigenous Australians’ health and wellbeing (Hollinsworth 2006; Briskman 2014). As the 2020 Closing the Gap Report indicates, current life expectancy for Aboriginal Australians involves the intersectionality of social determinants in which they are disadvantaged such as income, housing, education and employment, all of which are ‘estimated to be responsible for at least 34 per cent of the health gap between Indigenous and non-Indigenous Australians’ (Briskman 2014; Australian Government 2020 n.p.).
Statistics released in 2018 indicated the mortality rate for Indigenous Australians is approximately 1.7 times greater than for non-Indigenous Australians and the initiatives implemented by the Federal Government to close the mortality gap between the two groups is not on target to reach its’ objectives by 2031 (Australian Government 2020). Disadvantage created by institutionalised racism since colonisation concerning Aboriginal and Torres Strait Islanders is apparent in every area of Australian life and is often exacerbated by changing political policies and media discourses.
The Australian conservative media still perpetuate racist thinking, which would not exist if cultural responsiveness, white habitus and anti-racist practice was occurring across the board. The media provoked controversial public debate, involving the proud, highly accomplished Indigenous Australian Football League (AFL) player; Adnyamathanha man, Australian of the Year in 2014, Adam Goodes, divided the nation when between 2013 and 2015 he publicly stood against racism and freely expressed his indigeneity. Several examples of institutionalised racism from non-Indigenous media commentators Adam Bolt, Sam Newman and Alan Jones occurred, and as Waleed Aly pointed out facts were altered to support their racist views (Begone Abbott 2015; The Weekly 2015; Whoknowsuknow 2015). Various media outlets touted Goodes as a ‘sook’, ‘whinger’, ‘cry baby’ and it was stated he was ‘playing the race card’ (Guatum 2019, p. 17). When, in the AFL Indigenous Round, which recognises and celebrates Indigenous culture, Goodes performed a celebratory war cry dance, the situation escalated to the extreme where every time he played football he was loudly booed by the crowd in what de Souza (2018, p. 460) described as a ‘sonic barometer that measures who is accepted and who is rejected.’ Acting within a model of cultural responsiveness requires critical self-reflection, recognition of the impact social structures have on individuals, asks questions, allows for critical examination of the structures which create oppression and permits the challenging of those structure (Green, Bennett & Batteridge 2016).
A culturally responsive approach therefore would have de-escalated the situation by commentators asking questions in order to perceive the situation from Goodes perspective, whilst critically reflecting on their own behaviour, thereby showing respect and affirming the multicultural diversity which exists in Australia. Instead, inflammatory, derogatory, racist and ignorant statements were made which impacted on Goodes’ health (BBC HARDtalk 2020). A culturally safe response would have also encompassed being aware not only of Aboriginal history but of Goodes’ personal history because when he was racially vilified by a young girl and then subjected to the persistent media coverage and booing from crowds it all not only shocked him but triggered racist traumatic memories of childhood experiences (Green, Bennett & Betteridge 2016; BBC HARDtalk 2020). Whilst Eddie MacGuire, in his role as media commentator and Collingwood Football Club president, initially supported Goodes, both MacGuire and former Victorian Premier, Jeff Kennett publicly criticised Goodes’s dance as being deliberately provocative and defended the crowd’s booing as being an acceptable response (de Souza 2018). The persistent booing and various criticisms which surrounded Goodes created a toxic workplace which pushed Goodes into a deep depression, resulting in him walking away from the sport he loved in 2015, for the sake of his mental health (BBC HARDtalk 2020).
In 2016 Australians spoke 300 languages and whilst the country purports to embrace multiculturalism, ongoing debate has occurred for decades amongst the media, politicians and academics concerning the concept and implementation of a multicultural society (Australian Bureau of Statistices 2016; Koleth 2010). Fear-based conservatives like John Howard and Pauline Hansen have been concerned that a true multi-cultural Australia will undermine the existing social structures and they have wanted to continue ‘preserving constructions of Australian nationhood and culture’ (Koleth 2010, n.p.). Yet, science has proven race is not a biological fact, but a social construct designed to have power over others who are different to the white majority (California Newsreel 2003), which is why anti-racist practice is useful in relation to dismantling institutional racism. Stemming from Critical Race Theory there is agreement that racism is a widespread oppressive social construct (Ladhani & Sitter 2020; Constance-Huggins 2019).
Anti-racist practice respects individual agency, whilst challenging and resisting injustices as it involves a commitment to creating ongoing equal opportunities for all that aligns with ‘equity of outcome’ (Berman & Paradies 2009, p.218). Given the multitude of culturally diverse individuals existing in Australia today, Australian society, as an evolving entity, needs to move beyond colonial based institutionalised racism due to the damage it has and continues to create. By utilising white habitus, cultural responsiveness and anti-racism to eliminate the racialisation of people and the othering that white Australians in powerful public positions currently use, all Australians can move into a future which is more dignified, respectful and equitable. As Social Work now holds the previously mentioned principles, values and ethics at its’ core, all Social Workers have a duty, responsibility and obligation to assist in educating, challenging and changing institutionalised racism in this country because whilst multiculturalism is something Australians claim to embody, statistically and historically speaking multiculturalism and embracing cultural diversity, is a concept, not a reality.
Bennett, B & Green, S 2019, Our voices: Aboriginal social work, Second edition., Red Globe Press, London.
Berman, G & Paradies, Y 2010, ‘Racism, disadvantage and multiculturalism: towards effective anti-racist praxis’, Ethnic and Racial Studies, vol. 33, no. 2, pp. 214–232, doi: 10.1080/01419870802302272.
Briskman, L 2014, Social work with indigenous communities: a human rights approach, 2nd ed., The Federation Press, Annandale, NSW.
Constance-Huggins, M 2019, ‘Critical Race Theory in Social Work Education’, Critical Social Work, vol. 13, no. 2, doi:10.22329/csw.v13i2.5861.
de Souza, P 2018, ‘What does racial (in)justice sound like? On listening, acoustic violence and the booing of Adam Goodes’, Continuum (Mount Lawley, W.A.), vol. 32, no. 4, pp. 459–473, doi: 10.1080/10304312.2018.1488524.
Emirbayer, M & Williams, E 2005, ‘Bourdieu and Social Work’ Social Service Review, vol. 79, no. 4, pp. 689–724, doi:10.1086/491604.
Gautam, A 2019, ‘The monstrous other: Adam Goodes and the colonial legacy of “terra nullius”’ Social Alternatives, vol. 38, no. 4, pp. 16–20. ISSN: 0155-0306
Green, S, Bennett B & Betteridge S 2016, ‘Cultural Responsiveness and Social Work – a Discussion’ Social Alternatives, vol. 35, no. 4, pp. 66–72, viewed 4 November 2020, http://search.proquest.com/docview/1918326828/.
Hollinsworth, D 2006, ‘Race and Racism in Australia’, 3rd ed., Thomson Social Science Press, South Melbourne.
Sherwood, C, Osmond, G & Phillips M 2020, ‘Aboriginality, Racial Discourse and Football Media in 20th-century Queensland’, Journal of Australian Studies, vol. 44, no. 1, pp. 97–113, doi: 10.1080/14443058.2019.1668821.
Springer, R 2007, ‘A Nightmare of the Neocolonial Kind: Politics of Suffering in Howards’ Northern Territory Intervention, Borderlands e-journal, vol. 6, no. 2, Nuclear Territory News, viewed 4 November 2020, http://www.borderlands.net.au/vol6no2_2007/stringer_intervention.htm
Vanidestine, T & Aparicio, E 2019, ‘How Social Welfare and Health Professionals Understand “Race,” Racism, and Whiteness: A Social Justice Approach to Grounded Theory’ Social Work in Public Health, vol. 34, no. 5, pp. 430–443, doi:10.1080/19371918.2019.1616645.
Walter, M, Taylor, S, & Habibis, D 2011, ‘How White is Social Work in Australia?’ Australian Social Work: On Australian Indigenous Social Work and Social Policy Part 1, vol. 64, no. 1, pp. 6–19, doi:10.1080/0312407X.2010.510892.
Young S 2008, ‘Indigenous Child Protection Policy in Australia: Using Whiteness Theory for Social Work’, Sites: New Series, vol 5, no 1, viewed 4 November https://doi.org/10.11157/sites-vol5iss1id82
Race as a social construct came into being alongside capitalism. When European colonists arrived in Australian with their ethnocentric ideology, racist foundations became the building blocks upon which inequity and institutions were built. As a result, the trauma and inequality created for Aboriginal and Torres Strait Islanders by colonialism has, and continues to, impact detrimentally on their health and well-being despite Governments expending large sums of money on programs and services to close the gap between Indigenous and non-Indigenous outcomes in relation to health. The colonialist mentality of racism in Australia towards Aboriginal and Torres Strait Islander people is maintained by three main forms of racism; institutionalised, interpersonal and internalised. Institutionalised racism, particularly within the health system, is creating a plethora of inequity issues which are resulting in high mortality rates amongst Aboriginal and Torres Strait Islander communities.
The publication of The Origin of Species, written by biologist and philosopher Charles Darwin in 1859, led to eugenics, phrenology, ethnocentricity and Social Darwinism, and subsequently race and racism began. Darwin’s theory of evolution and natural selection proposed that differences between human beings, such as skin colour, equated to different races of human beings existing and therefore those who did not have the same attributes as Europeans were classified as being of a different species, or race (Hollinsworth 2006, p.32). His theory added scientific credence to, and fueled the fire of, the political, social and medical discourses being espoused by Herbert Spencer, an English sociologist, biologist and prominent liberal political theorist (Hollinsworth 2006, p.32). Darwin’s theory led to Social Darwinism being established within European society (Hollinsworth 2006, p.32). Race and racism was therefore founded on the politics of eugenics and the medical and political discourses which spread globally during the end of the nineteenth century and into the twentieth century (Bastos, Harnois & Paradies 2016, p.209). Eugenics is the science of controlling breeding within populations so there is an increasing manifestation of the required genetic characteristics (Galton 1904, p.1). Indigenous Australians were seen by European colonists to be situated at the very bottom of a hierarchical ladder which Europeans existed at the summit of (Germov & Poole 2007, p. 284). This mentality was known as ethnocentricity which is when a belief exists that your own culture or ethnic group is superior to another (Bizumic & Duckitt 2012, p.887). It was also seen by Europeans that Indigenous people were inferior biologically due to the pseudo-scientific theory of phrenology which equated skull size and shape as being able to determine a person’s character (Germov & Poole 2007, p. 284). With eugenics, phrenology and ethnocentricity firmly implanted in the minds of the colonists who invaded Australia, it takes little sociological imagination to understand why European colonists behaved as they did towards Aboriginal and Torres Strait Islander people.
When the invasion of Australia by the British occurred in 1770 they brought with them fixed mindsets of capitalism and Social Darwinism and the colonisation of Australia began. Colonialism relates to a system being implemented whereby an individual or group of individuals seek to dominate others (Horvath 1972, p.46). Sociological theorist Pierre Bourdieu referred to colonialism as a forceful system of oppression based on racist beliefs which seeks to reorganise social kinships and at the same time establish a crossbred society (Go 2013, p. 49).Colonialism is also a powerful and aggressive action taken by people to possess land and exploit it, along with the Indigenous people who occupy that land, with no regard to the original inhabitants, their culture or their existing laws (Horvath 1972, p. 46). Karl Marx believed this type of domination occurs out of an economic basis and is a symptom of capitalism (Horvath 1972, p.46). Horvath states colonisation creates and perpetuates social injustice (Horvath 1972, p.46). Colonists were of the fear-based view that Aboriginal and Torres Strait Islander people were savages who were dangerous, yet childlike (Hollinsworth 2006, p.33).As such, great measures to establish and maintain superior paternalistic power and control over Indigenous Australians began because of unconsciously based scientific racist beliefs (Hollinsworth 2006, p. 34). This fear-based power and control continued to have a stronghold in Australia into the later part of last century (Hollinsworth 2006, p. 34). Because of Darwin’s theory of natural selection, Indigenous Australians were seen to be a separate race of people who colonists believed were destined to die out anyway (Hollinsworth 2006, p. 35).It was often the situation that anyone who protested the horrendous treatment Indigenous people received whilst colonisation was occurring, were met with rebuttal (Hollinsworth 2006, p. 35).It was also seen to be worthy of celebration by colonists, not lamentation, that the extinction of an inferior race was occurring, with their help (Hollinsworth 2006, p. 35). The attempted assimilation which occurred of trying to change the genetics of Indigenous Australians was a direct result of eugenics. It was these underlying beliefs colonisers held which established Australia’s institutions and created the systemic racism which still exists within those institutions today.
Institutionalised racism lays at the core of all of Australia’s systems and is closely linked with capitalism. Race and racism in Australia can be understood as being maintained institutionally when looked at through the sociological lens of Foucault’s theory that governmental control occurs via the power maintained in institutional systems, which then becomes internalised normality within society (Germov & Poole 2007, p. 287).From a Marxists perspective Governments would not want to change the existing institutionalised racism because to do so would alter the balance of power which would no longer serve the interests of capitalism (Germov & Poole 2007, p. 287). Racism is defined as a discriminatory dispersal of chances, assistance or capital implemented by the dominant culture over minority groups of different race or ethnicity (Paradies, 2018, 0.42 – 1.44). Institutionalised racism has been defined as having its basis in historical social scenarios which continues due to frameworks that preserve prior discriminations (Jones 2001, p.1212). Institutionalised racism is often seen to be legalised and lays within the policies and practices of institutions, whilst also being apparent when procrastination occurs, instead of action, in relation to needs not being met (Jones 2001, p.1212). Evidence shows that racism, whilst not a set target in the Close the Gap Report 2008 (Parliament of Australia undated, p. n/a), has been recognised by the Federal Government in the Close the Gap Report Review 2018 (Australian Human Rights Commission 2018, p.3) and in the National Aboriginal and Torres Strait Islander Health Plan 2013-2023 (Australian Government Department of Health 2013, p.8). Due to institutionalised racism, which has become the societal norm, many Australians do not see their unconsciously conditioned biases perpetuate not only the racism the country’s systems were built on, but also that they serve to maintain the inequality between Indigenous and non-Indigenous Australians which began over two hundred years ago.
Interpersonal racism, along with institutionalised racism and deficit discourses within politics and the media are having an adverse effect on the mental and physical health of Indigenous Australians. Interpersonal racism can be conscious or unconscious and appears in society by way of stereotyping, lack of service, ignoring, lack of respect and devaluation (Jones 2001, p.1213).Institutionalised racism, combined with interpersonal racism lead to internalised racism, which involves taking on the limiting beliefs about oneself which have been projected by the dominant culture onto the minority group (Jones 2001, p. 1213).Internalised racism can also lead to a lack of self-worth, lack of belief in peers and in one’s self (Jones 2001, p. 1213). The general dominant political and media discourse in Australia is increasing the inequality many minority groups encounter from the dominant culture (Hollinsworth 2006, p. 246). Since 1996, when the Howard Government came into power, there has been a steadily growing manufactured erosion of social justice and equal rights occurring in Australia via an official discourse being implemented through laws based on fear and envy (Hollinsworth 2006, p 246). This stance will only lead to increasing inequality, endangering existing social structures and possibly result in an increase in violence occurring (Hollinsworth 2006, p. 246). Combined with these deficit discourses created by non-indigenous media and politicians in Australia towards Indigenous Australians, racism has been found to be detrimental to Aboriginal and Torres Strait Islanders health as they all impact adversely psychologically, emotionally and in relation to their overall social wellbeing.
Perceptions of race and racism within Australian have been shown, through a variety of micro and macro level methods, to reveal health care barriers exist for Indigenous Australians which do not exist for non-Indigenous Australians. Systemic racism not only has detrimental outcomes such as depression, suicide, anxiety and post-traumatic stress disorder for Indigenous Australians, but it also creates significant economic impacts on society (Paradies 2016, p.1). In 2016 it was estimated that racial discrimination cost the Australian economy approximately 37.9 billion dollars per annum (Paradies 2016, p.1). A study conducted during 2012 and 2013 revealed thirty percent of Aboriginal and Torres Strait Islander people suffer from extreme psychological and emotional occurrences of depression or anxiety (Australian Institute of Health and Welfare 2015, p. 71). This figure is extraordinarily high when one considers that Indigenous Australians make up only three percent of the national population (Bastos, Harnois & Paradies 2016, p.211). Further, it was revealed in 2012 that Indigenous Australians experience higher rates of suicide than non-Indigenous Australians with deaths being predominantly higher for males between the ages of twenty-five and twenty-nine (Australian Bureau of Statistics 2012, p. n/a). The statistics of deaths based on a scale of one hundred thousand per population for this age group show that non-Indigenous male deaths by suicide peak at twenty percent and Indigenous males peak at ninety percent (Australian Bureau of Statistics 2012, p. n/a). In 2014 a General Social Survey was conducted to determine the degree racial discrimination intersects with other areas of discrimination such as, gender, sexuality, class and age within Australia, in creating access barriers to health care (Bastos, Harnois & Paradies 2016, p.209). The results concluded perceived racism was a major factor creating a barrier in accessing health care, particularly mental health (Bastos, Harnois & Paradies 2016, p.216). There is ample available research which indicates that the social construct of race is responsible for the ongoing high mortality rates occurring within Aboriginal and Torres Strait Islander communities. Racism in its various forms is not only creating barriers to accessing health care but creating ongoing psychological and emotional distress for a large percentage of Indigenous Australians.
According to sociologists, Australia has moved into a time of post-modernity and post-colonialism, but the evidence clearly shows the social construct of race and the racism which stems from it continues to be maintained by way of institutionalised racism. Post-colonialism came into being late in the twentieth century (Eagleton 2011, p. 222).It is defined as a time when physical violence is no longer being perpetrated to take land (Hollinsworth 2006, p.246). This may be the situation; however, it appears that a new form of racism has taken the place of the past brutal dispossession, assimilation and genocide. Known as new racism, this form revolves around the structure and appearance of racism in relation to pecuniary and socio-traditional variances which exist between the overriding and minority cultures within a country (Germov & Poole 2007, p. 287).Post-colonialism studies look at the relationships between oppressors and oppressed existing in countries that have been colonised (Germov & Poole 2007, p. 287).Indigenous identity, which post-colonialism also concerns itself with, has been revealed via various institutional policies to have been manipulated to implement and validate dominant policies (Germov & Poole 2007, p. 288).Colonialism was rooted in racism and whilst many perceive both exist historically and are no longer apparent, both still exist within capitalism as the Western thinking of those in power continues to be based on the taking of other people’s land who are not in positions to stop them (Jureidini & Poole 2003, p.246). It is in the continuation of institutionalised racism and subsequent racist policies and practices, by those in power within the Westernised political system, that inequity continues to grow and create an ever-widening gap between capitalist politicians and those who they deem to be inferior.
Race and racism are social constructs designed by the political upper class in Europe in the late 1800s based on ethnocentricity. Institutionalised racism has created discrimination, exploitation, distress and inter-generational trauma which is still impacting on Aboriginal and Torres Strait Islander people. Whilst State and Federal Governments have spent voluminous sums of money on programs and services to bring about more equality between non-Indigenous and Indigenous Australians in relation to health, they have failed. Up until 2013 they did not recognise that systemic racism within Australian institutions is responsible for the lack of equity, agency, health issues, self-governance and self-determination Aboriginal and Torres Strait Islanders have been and still are experiencing.
Australian Government Department of Health 2013, National Aboriginal and Torres Strait Islander Health Plan 2013-2023, p. 8, viewed 18 October 2018 http://www.health.gov.au/natsihp
Bastos, J, Harnois, C & Paradies, Y 2018, ‘Health care barriers, racism, and intersectionality in Australia’, Social Science & Medicine, vol. 199, pp. 209 – 218. doi: 10.1016/j.socscimed.2017.05.010
Bizumic, B & Duckitt, J 2012, ‘What Is and Is Not Ethnocentrism? A Conceptual Analysis and Political Implications’, Political Psychology, vol. 33, no. 6, pp.887–909. doi:10.1111/j.1467-9221.2012.00907
Eagleton, T 2011, Why Marx was right, Yale University Press, New Haven.
Elias, A & Paradies, Y 2016, ‘Estimating the mental health costs of racial discrimination’ BMC Public Health, vol.16, no. 1(1), p.n/a, doi: 10.1186/s12889-016-3868-1
Galton, F 1904, ‘Eugenics: Its Definition, Scope, and Aims’, American Journal of Sociology, vol. 10, no. 1, pp.1–25. doi: 10.1086/211280
Germov, J & Poole, M 2007, Public sociology: an introduction to Australian society, Allen & Unwin, Crows Nest, N.S.W..
Go, J, 2013, ‘Decolonizing Bourdieu: Colonial and Postcolonial Theory in Pierre Bourdieu’s Early Work’, Sociological Theory, vol. 31, no. 1, pp.49–74. doi: 10.1177/0735275113477082.
Hollinsworth, D 2006, Race & racism in Australia 3rd ed., Thomson Social Science Press, South Melbourne.
Horvath, R 1972, ‘A Definition of Colonialism’, Current Anthropology, vol. 13, no. 1, pp.45–57. doi:10.1086/201248
Jones, C 2000, ‘Levels of racism: A theoretic framework and a gardener’s tale’, American Journal of Public Health, vol. 90, no. 8, pp.1212–1215. Doi:10.2105/AJPH.90.8.1212
Jureidini, R. & Poole, M 2003. Sociology: Australian connections, 3rd edn, Allen & Unwin, Crows Nest, N.S.W.
Paradies, Y 2013. ‘A Culturally Respectful and Non-Discriminatory Health System’, Viewed 26 August 2018, https://vimeo.com/11864669